 This website is best viewed
This website is best viewed
using the horizontal display on
your tablet device.
This site is intended for Canadian
Healthcare Professionals only.
Healthcare Professionals only.
ENGLISH
FRANÇAIS
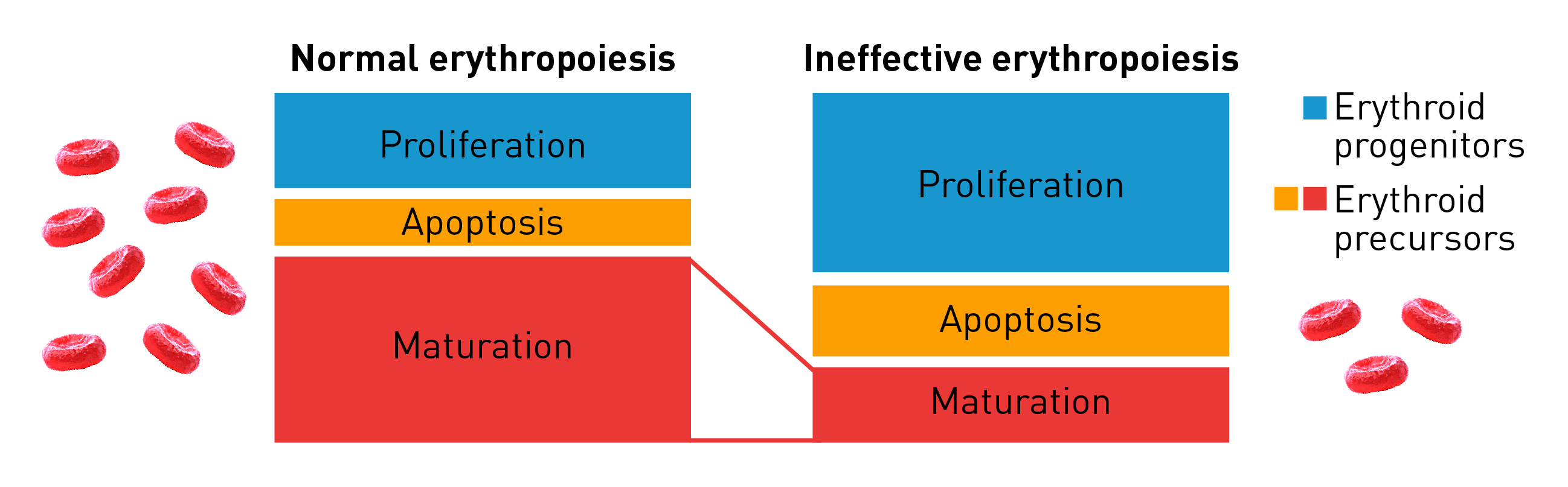
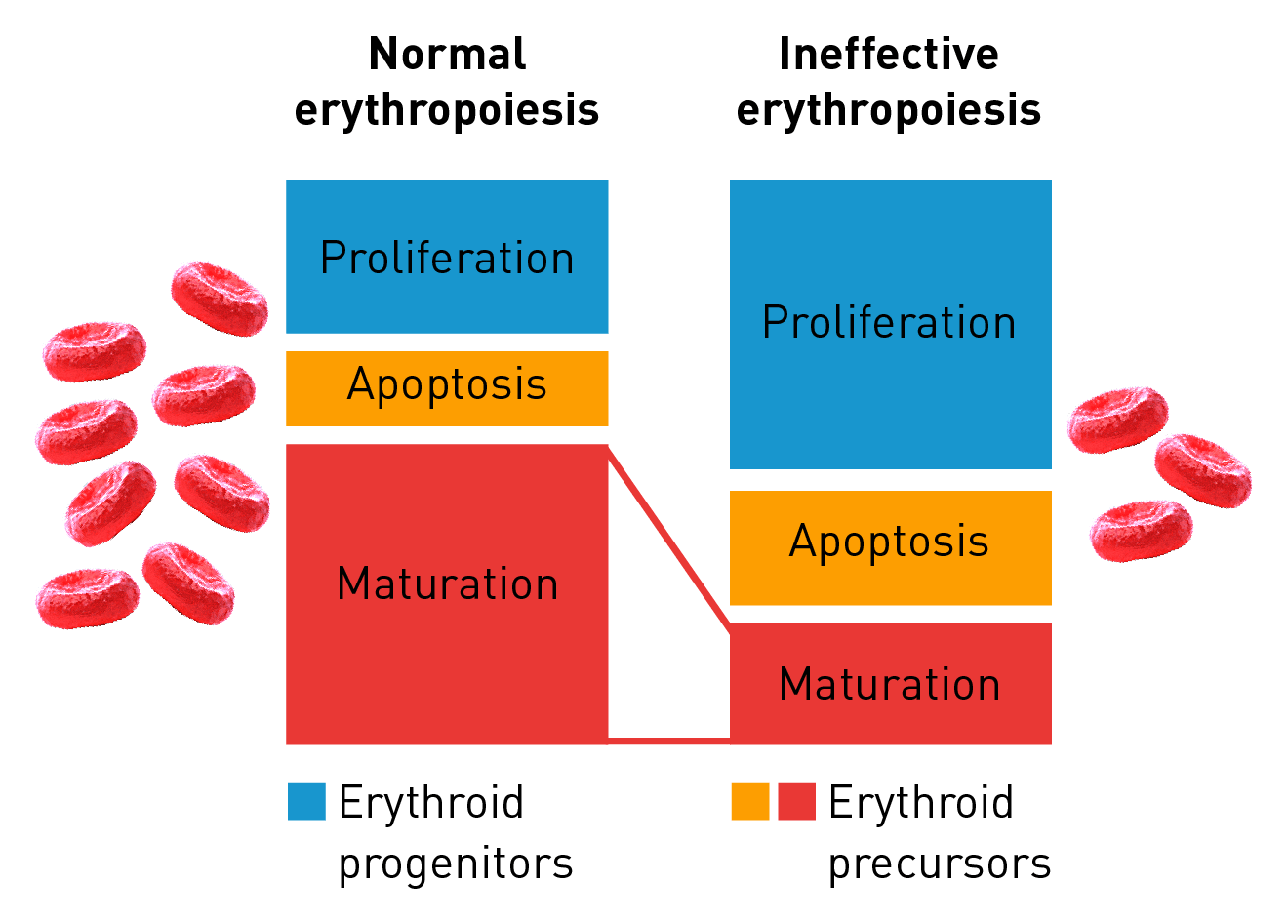
Characteristics of ineffective erythropoiesis
Normal erythropoiesis proceeds with tight regulation of maturation and apoptosis to maintain red blood cell homeostasis and normal oxygen levels.4 However, ineffective erythropoiesis is an ongoing pathological state where increased erythroid proliferation is unable to restore red blood cell count due to increased apoptosis of immature erythroid cells and impaired late-stage maturation.1,4
Implications of ineffective erythropoiesis
Chronic anemia
- Ineffective erythropoiesis may result in chronic anemia and its associated symptoms, such as cardiac failure, fatigue, dyspnea, tachycardia, hypotension, low body temperature and an enlarged spleen4-6
Iron overload
- Hepcidin, an iron metabolism regulator, may be suppressed in the liver due to ineffective erythropoiesis, leading to unrestrained intestinal iron uptake1
- Increased iron levels may result in the saturation of plasma transferrin and the accumulation of non-transferrin-bound iron in the body, creating iron deposits in various organs1,7
- This results in a range of clinical complications including pituitary damage, hyperthyroidism, liver disease, heart failure and diabetes6,7,8
Abnormal erythroid marrow expansion
- Bone deformities may appear in the skull and face, as observed in patients with thalassemias8
Hypercoagulability
- This state is linked to a high prevalence of thromboembolic and cerebrovascular events associated with ineffective erythropoiesis8
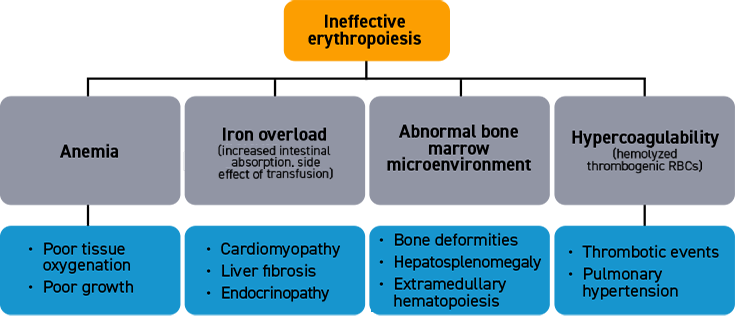
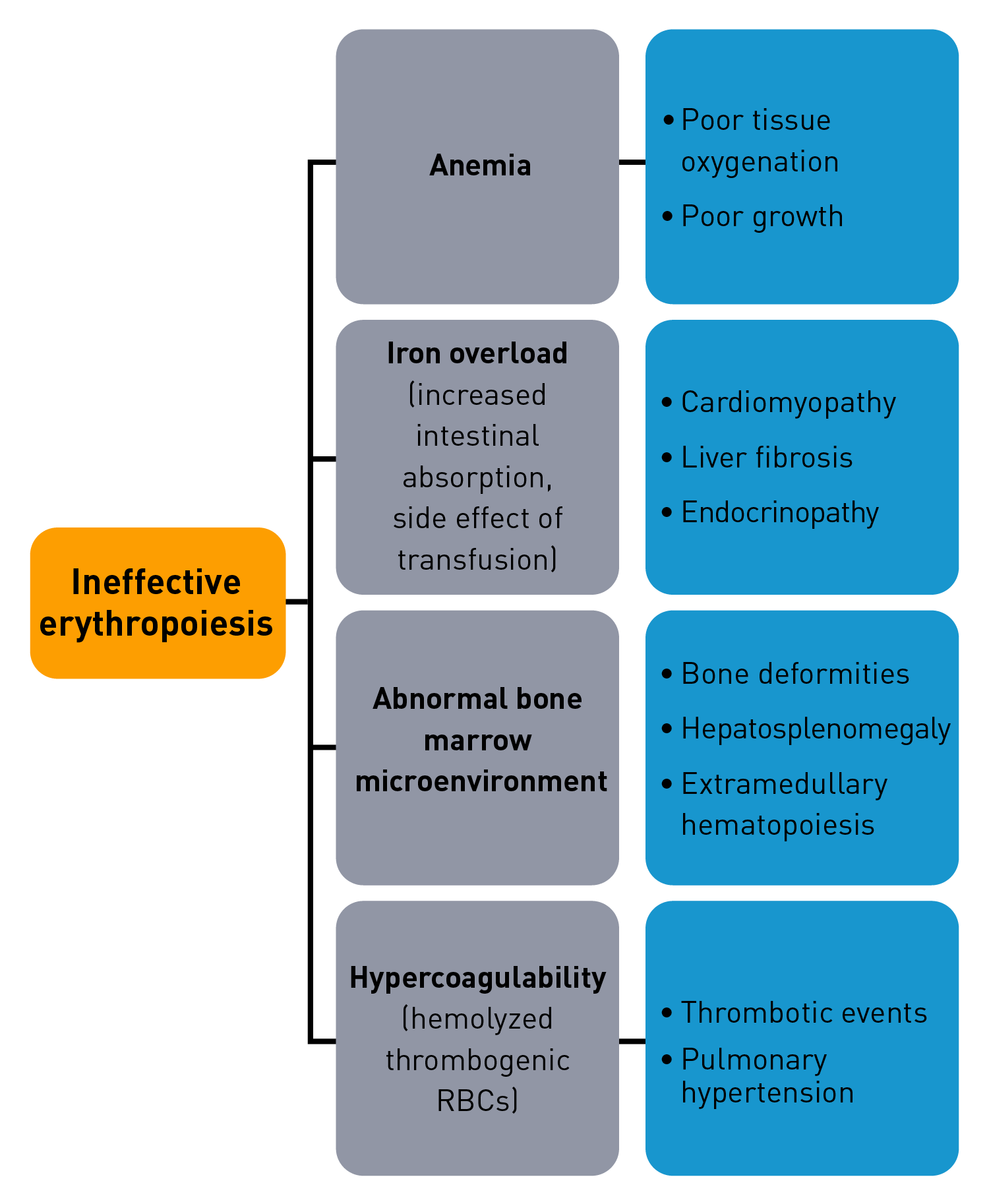
Ineffective erythropoiesis contributes to a variety of symptoms and complications that are characteristic of certain hematological disorders1
Erythroid maturation defects in hematological diseases
Erythroid maturation defects (EMDs) form the underlying mechanism of ineffective erythropoiesis. EMDs may induce changes in cellular and molecular signalling pathways linked to ineffective erythropoiesis and contribute to chronic anemia observed in certain hematological diseases.1
Reduced HSP70 and GATA-1 concentrations
HSP70 and GATA-1 form complexes to promote erythroid differentiation and maturation. HSP70 is regulated by EPO and is important to protect free GATA-1 factors from cleavage. However, in diseases such as β‑thalassemia and MDS, low concentrations of HSP70 – GATA-1 complexes were observed due to reduced EPO concentrations. The free, unprotected GATA-1 factors then become prone to cleavage and result in decreased erythroid differentiation and maturation, leading to ineffective erythropoiesis.9
Elevated TGF-β concentrations
TGF-β superfamily members may produce EMDs that cause dysregulation of signalling pathways in diseases such as sickle cell anemia and MDS. Elevated levels of selected TGF-β superfamily members have been observed in patients with sickle cell anemia.10
In bone marrow samples from patients with MDS, altered TGF‑β superfamily signalling, mediated by the over-activation of the SMAD pathway, has been shown to contribute to ineffective erythropoiesis and chronic anemia.11
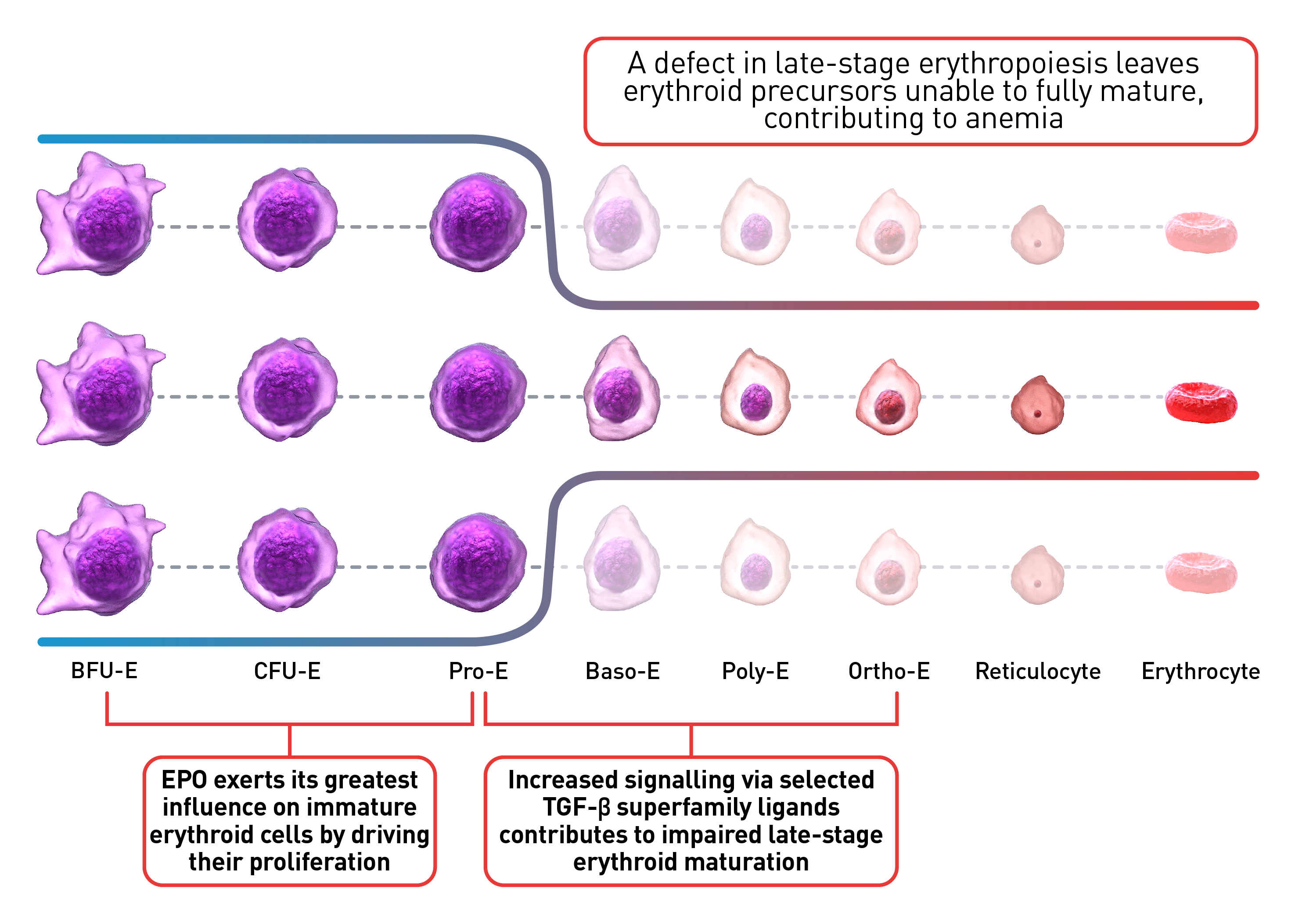
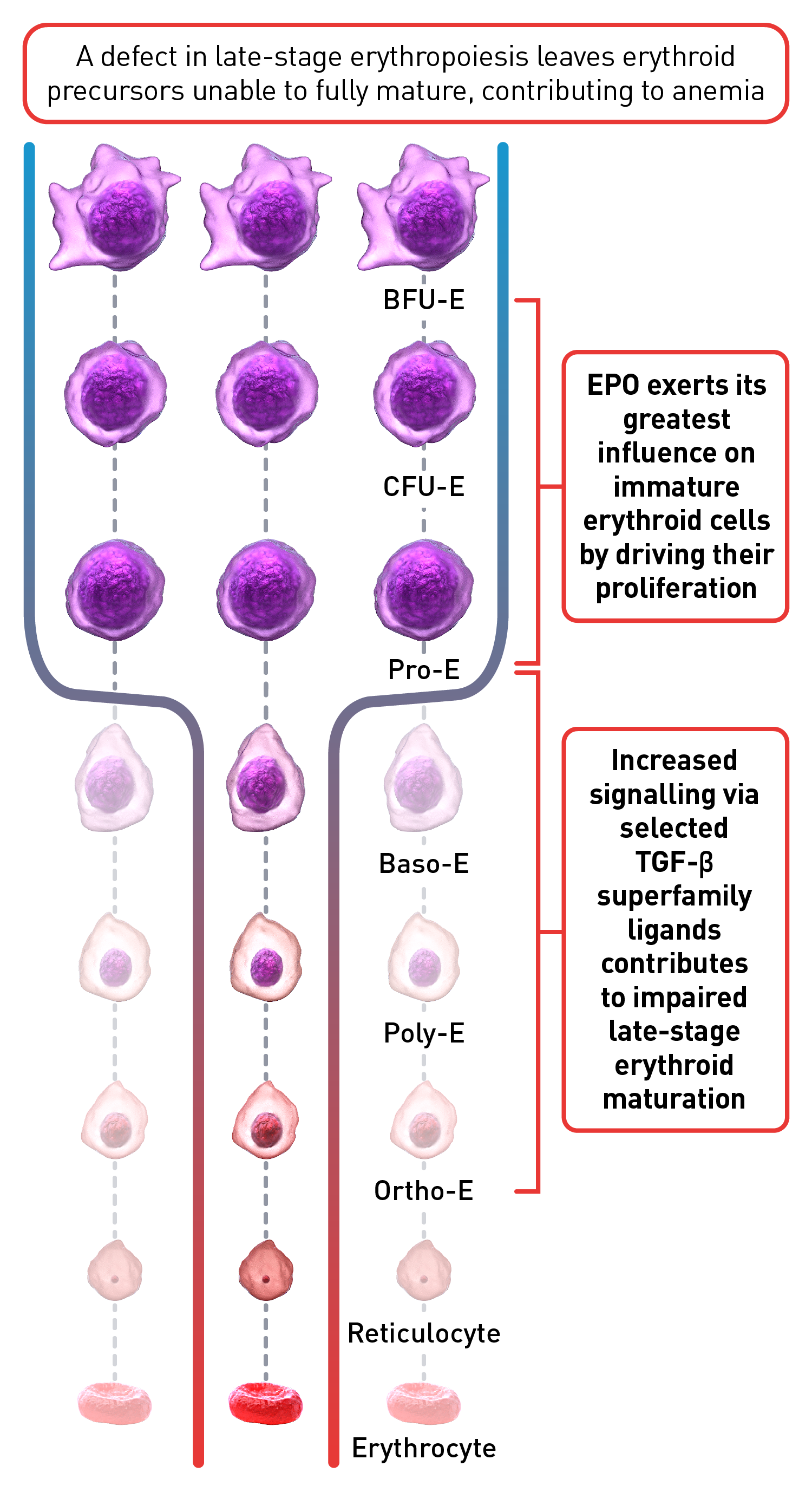
The process of erythroid maturation involves a complex network of transcription factors and epigenetic regulators. EPO is the key regulator of early-stage erythropoiesis, whereas some members of the TGF‑β superfamily are involved in the regulation of late-stage erythropoiesis.10,12 Overactivation of TGF‑β signalling, mediated by selected SMAD proteins, is implicated in impaired erythroid maturation, contributing to EMDs and ineffective erythropoiesis.12
Research into the molecular mechanisms of ineffective erythropoiesis revealed that EMD is implicated in the pathogenesis of anemia in certain hematological disorders.9
RBC: Red blood cells, HSP: Heat shock protein, Baso‑E: Basophilic erythroid, BFU‑E: Burst-forming unit-erythroid, CFU-E: Colony-forming unit-erythroid, EMD: Erythroid maturation defect, EPO: Erythropoietin, Ortho-E: Orthochromatophilic, Poly‑E: Polychromatophilic, Pro‑E: Proerythroblasts, TGF: Transforming growth factor.
 This website is best viewed
This website is best viewed
using the vertical display on
your mobile device.